
{kind=link}
6. Surgical Interventions
6.1. Hematoma Evacuation
6.1.1. MIS Evacuation of ICH
Referenced studies that support recommendations are summarized in Data Supplements 55 and 56.
Synopsis
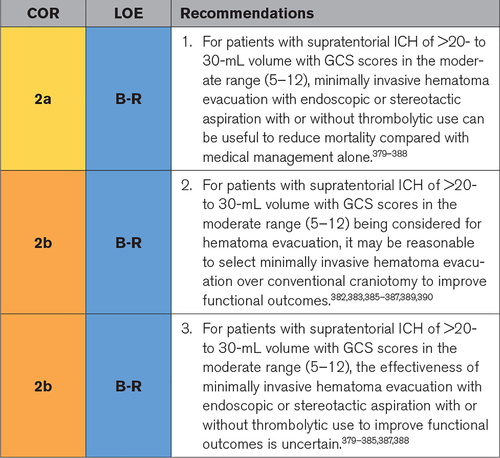
MIS for supratentorial ICH has the appeal of relieving hematoma volume, reducing perihematomal edema, and, compared with conventional craniotomy, minimizing disruption of healthy brain tissue. Therefore, enthusiasm for MIS techniques to treat moderate to large ICHs during the acute phase seems intuitive. However, results from large randomized clinical trials have not been definitive.379–388,391,392 The present guideline uses primarily data from the largest RCT of MIS (MISTIE III),381 meta-analyses of trials comparing MIS with conventional craniotomy and standard medical care,379,380,382–390,393–395 and smaller RCTs.391,392,396–412 The majority of clinical trials have used ICH volume thresholds of >20 or >30 mL as an inclusion criterion. As a primary recommendation, minimally invasive hematoma evacuation with endoscopic or stereotactic aspiration, with or without thrombolytic use, is safe and may be useful to reduce mortality. Although it may also improve functional outcomes, the LOE for this is lower. Compared with craniotomy, the mortality benefit of MIS is uncertain, although the literature supports that MIS may be considered to improve functional outcomes compared with conventional craniotomy. MIS interventions require surgeon and center skill and experience as the basis for these recommendations.
Recommendation-Specific Supportive Text
- Mortality, a prespecified secondary analysis in MISTIE III, was significantly lower in the MIS group compared with the standard medical care group at 7, 180, and 365 days, although the trial was neutral on the primary outcome (functional outcome benefit).381 Although smaller, likely underpowered RCTs did not always show a mortality benefit for MIS,392,400,401,406,408 most meta-analyses comparing stereotactic puncture or endoscopic drainage with standard medical care reported significantly decreased odds of death with any MIS compared with standard medical care.380,382,386–390,394 Multiple safety end points were addressed in the MISTIE III trial, including symptomatic hemorrhage within 72 hours after last dose of alteplase and bacterial brain infection, which were similar between groups, indicating that stereotactic aspiration with thrombolysis appears to be safe.381 SAEs at 30 days were significantly lower in the MIS group versus the standard medical care group. Only asymptomatic bleeding was higher in the MIS versus the standard medical care group (32% versus 8%). Other RCTs and meta-analyses confirm no significant difference in safety end points (brain rebleeding after treatment and infection) for endoscopy and stereotactic aspiration/craniopuncture techniques compared with standard medical care or craniotomy.391,398,400,405,406,408,411–413 Most RCTs enrolled patients <80 years of age, although age did not modify the effect of surgery except in 1 meta-analysis in which improved outcomes from any surgery for ICH were found for patients 50 to 69 years of age.393
- Studies comparing MIS with conventional craniotomy have shown improved outcomes with a less invasive approach, raising the possibility that open craniotomy may damage more brain tissue while removing blood. Both small RCTs389,398,399,411,412,414 and all meta-analyses of either clinical trials alone or combined with observational studies from different settings comparing stereotactic puncture or endoscopic drainage with craniotomy have shown significantly decreased odds of functional dependence (or combined with death) and increased odds of good functional outcome with MIS.383,385–387,389,390,394,395 A network meta-analysis suggested the highest ranking of favorable prognosis for stereotactic aspiration, followed by endoscopy, then craniotomy, and last standard medical care.382 RCTs comparing MIS with craniotomy have included patients with ICH volume >25 mL and time interval to surgery from <6 to 72 hours after presentation. In the early surgery study, MIS showed a functional outcome benefit compared with craniotomy only if the CTA spot sign was positive but also showed a higher risk of rebleeding.399
- Many small RCTs of MIS show a functional outcome benefit from MIS compared with standard medical care at follow-up times of 3 months to 1 year.391,392,396–399,401,403,408,412,413 In the MISTIE III trial, stereotactic aspiration plus irrigation with alteplase did not improve functional outcomes at 1 year compared with standard medical care in patients with ICH volume >30 mL.381 However, planned exploratory analyses of clot removal showed a significant association between extent of clot removal and both mortality and lower mRS score (0–3), specifically in those patients who achieved the surgical aim (end-of-treatment clot size ≤15 mL). Meta-analyses of this and smaller clinical trials and observational studies from different settings comparing stereotactic puncture or endoscopic drainage with standard medical care have shown improved functional outcomes (alone or together with survival) with MIS.379,380,382–390,394 Most RCTs included only ICH volume >20 mL, although several included ICH volumes as low as 10 mL. One meta-analysis found that MIS was most beneficial for patients with hematoma volume between 25 and 40 mL and with a GCS score ≥9,387 whereas MISTIE III and 2 other meta-analyses found that hematoma volume did not modify the effect of surgery.379,381,384
Knowledge Gaps and Future Research
- Current evidence does not support specific recommendations for selecting candidates for surgery. A priori analyses focusing on clinical details, hematoma volume, patient age, GCS score (baseline clinical severity), and follow-up timing would inform future clinical trial design and recommendations.
- RCTs of MIS have not addressed a priori questions about timing of surgery and intent to stabilize ICH before surgery. Optimal time to surgical treatment with MIS remains a controversial issue primarily because of the risk of rebleeding, although reducing hematoma volume early (<12 or 24 hours) may reduce secondary brain injury and improve outcomes with no effect on bleeding risk as suggested by observational data. Several RCTs are underway that will address aspects of these questions.
- Although a functional outcome benefit of MIS compared with conventional craniotomy is reported for many RCTs, a mortality benefit is uncertain and may reflect the practice to perform craniotomy but not MIS in deteriorating patients. Most small RCTs are underpowered and did not show a mortality benefit of MIS compared with craniotomy; however, most meta-analyses of smaller clinical trials and observational studies comparing stereotactic puncture or endoscopic drainage with conventional craniotomy showed significantly decreased odds of death with MIS.
- Currently, no adequately powered clinical trial data compare different devices for MIS in ICH. Although surgeon experience and ability to achieve adequate hematoma removal with low rebleeding risk and acceptable outcomes may prove superior to a single technique, ongoing innovation with the development of new surgical devices will require comparisons of endoscopic and stereotactic techniques with thrombolysis and with potential for intrahematomal delivery of therapeutic agents. Ongoing RCTs will add useful data to these questions.
6.1.2. MIS Evacuation of IVH
Referenced studies that support recommendations are summarized in Data Supplements 57 through 62.
Synopsis
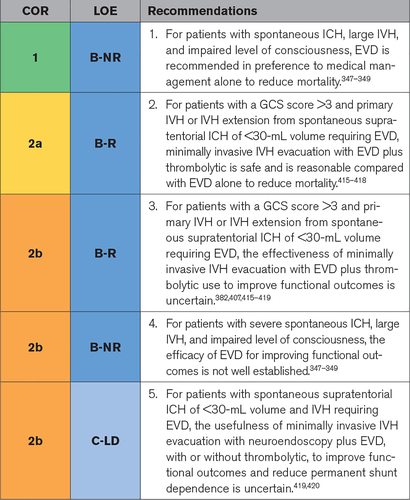
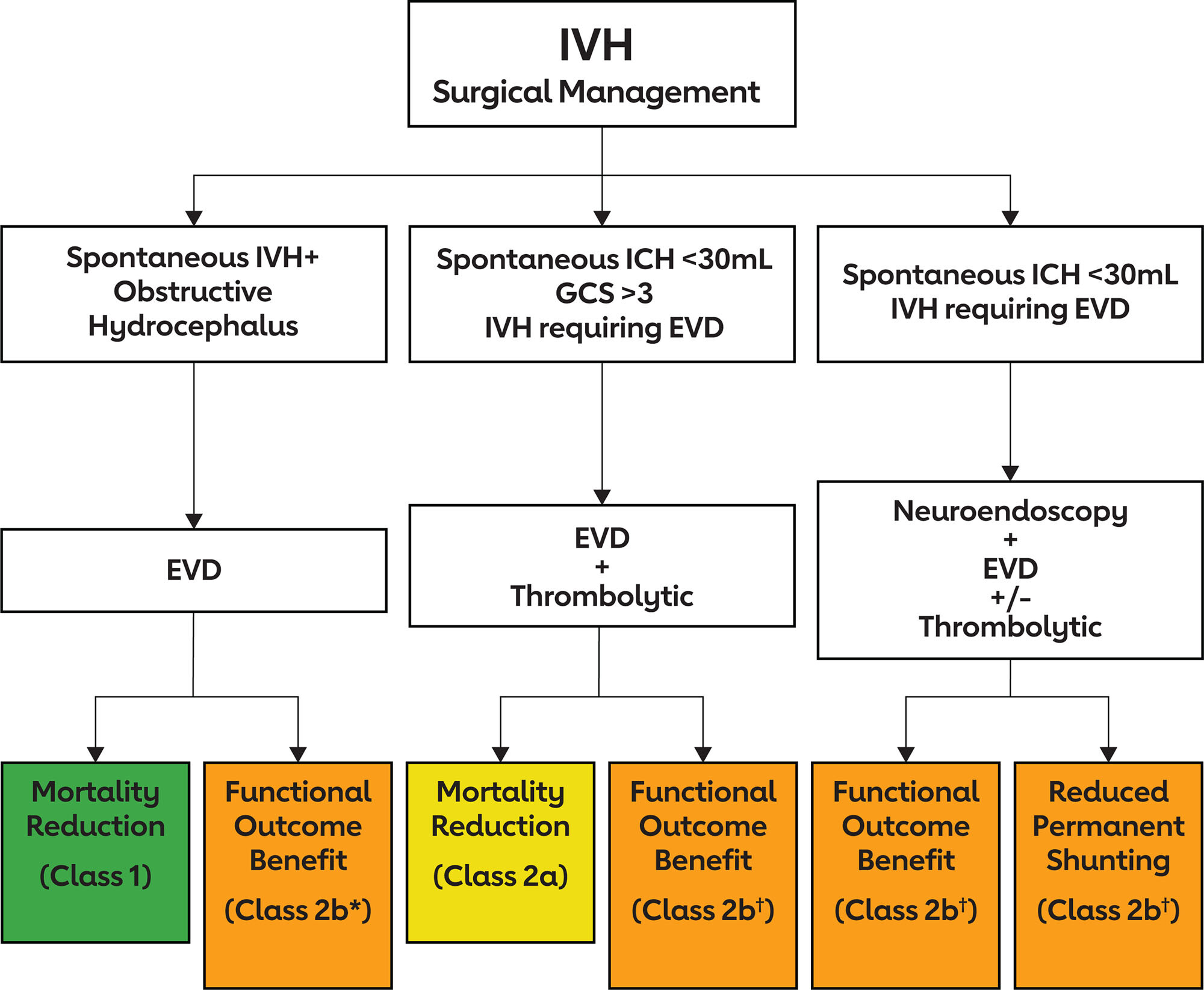
Intraventricular extension of ICH occurs in 30% to 50% of patients with ICH and predisposes to the development of hydrocephalus in approximately half of patients.421 IVH predicts a worse prognosis secondary to increased IVH volume and blood breakdown products that promote inflammatory meningitis and hydrocephalus.126 Insertion of an EVD to treat intracranial hypertension and remove blood products improves survival.347–349 The addition of thrombolytic irrigation with alteplase or urokinase hastens intraventricular clot removal and results in further mortality reduction.416,422 The current recommendations (illustrated in Figure 3) are based primarily on data from the largest RCT of intraventricular thrombolysis (IVT; CLEAR III [Clot Lysis: Evaluating Accelerated Resolution of Intraventricular Hemorrhage]),416 systematic reviews or meta-analyses of trials comparing (1) EVD with and without IVT with conservative treatment349 and (2) IVT with either EVD plus saline or EVD alone,415,417,418 and several smaller RCTs.356,423–425 As a primary recommendation, EVD with IVT is safe and improves survival in patients with clinical hydrocephalus and reduced level of consciousness compared with EVD alone (or with saline irrigation). However, the benefit of EVD to improve functional outcomes is uncertain. Other interventions studied for removing large volumes of IVH and reducing permanent shunt dependence include controlled lumbar drainage combined with IVT and targeted intraventricular neuroendoscopy.
Recommendation-Specific Supportive Text
- In patients with moderate to large IVH and higher clinical severity (defined in a propensity score–matched analysis as GCS score <13, ICH volume >11 mL, and Graeb score ≥7 [indicating moderate to severe IVH348]), EVD placement alone is associated with improved survival compared with conservative treatment.347–349 In a large retrospective analysis with propensity score matching, EVD use was associated with higher survival in patients with severe ICH as defined above, although not overall.348 A smaller retrospective analysis found a positive association of EVD alone with survival at hospital discharge in patients presenting with hydrocephalus and a GCS score >3 after adjustment for clinical severity.347 There were no age limits on these studies.
- In patients with IVH obstructing the third or fourth ventricle and small- to moderate-volume ICH (<30 mL), controlled irrigation with a thrombolytic agent such as alteplase or urokinase improves survival in patients with clinical hydrocephalus requiring a routinely placed EVD. Mortality, a prespecified secondary analysis in CLEAR III, was significantly lower in the EVD plus alteplase group compared with the EVD plus saline group at 180 days.416 Smaller RCTs also have shown a mortality benefit for IVT,356,423–425 and all meta-analyses of RCTs with or without observational data comparing EVD alone or with saline with EVD plus alteplase or urokinase reported significantly decreased odds of death with IVT.415,417,418 Multiple safety end points were addressed in CLEAR III, including symptomatic hemorrhage, which was not different between study groups. Both bacterial ventriculitis and SAEs were significantly less frequent in the alteplase group versus the saline-administered group, indicating that IVT appears to be safe.416 Other RCTs and meta-analyses confirm no significant difference in safety end points (rebleeding after treatment and ventriculitis) for IVT compared with EVD alone or with saline irrigation.
- It is not clear whether EVD plus IVT improves functional outcomes. In CLEAR III, EVD plus irrigation with alteplase did not improve functional outcomes at 180 days compared with EVD plus saline in patients with obstructive IVH and ICH volume <30 mL.416 However, a low proportion of participants achieved near-complete clot removal, and functional benefit was reported from removing greater amounts (>85%) of IVH volume. Alternatively, the absence of benefit of IVT on functional outcome in clinical trials might also be attributable to cerebral injury associated with parenchymal hemorrhage. CLEAR III included a high proportion of patients with thalamic ICH, a location with poor prognosis. In CLEAR III, a greater proportion of patients in the IVT arm had severe disability (mRS score 5) at 180 days, suggesting that mortality reduction occurred at the expense of severe morbidity. Meta-analyses of this and smaller clinical trials and observational studies comparing IVT to EVD (with or without saline) have shown heterogeneous effects on functional outcomes from IVT, depending on time of follow-up and functional outcome scale used.415,417,419,426 Most RCTs included patients up to 75 or 80 years of age. CLEAR III excluded patients with anticipated early withdrawal of life-sustaining therapies. For patients being considered for IVT, shared decision-making between physicians and family members is recommended to weigh mortality and functional outcome benefits with consideration of patient preferences.
- Compared with conservative treatment, there is uncertainty over whether EVD alone improves functional outcomes. In a systematic review of studies including patients with nontraumatic IVH secondary to ICH or subarachnoid hemorrhage and Graeb score >7, EVD alone was not associated with return to an independent lifestyle.349 In a large retrospective analysis with propensity score matching, EVD use was not associated with functional outcome at discharge.348 Subgroup analysis by several clinical severity factors found that patients receiving an EVD had more disability on the mRS compared with patients who did not receive an EVD. In this retrospective cohort, it is possible that patients who received an EVD were more severely disabled at presentation, thus requiring an EVD, versus those who did not. Moreover, patients who may have died without EVD placement also may have worse outcomes. A smaller retrospective analysis found a positive association between EVD alone compared with no EVD and good outcome at hospital discharge.347 However, retrospective studies are unable to evaluate unmeasured confounders that contribute to the decision to place EVDs in patients with IVH.
- Endoscopic surgery for hypertensive IVH combined with EVD with or without IVT has been studied in small RCTs and observational studies.419,420,427,428 Small RCTs have reported no significant difference in mortality rate, and 2 of them reported improved short-term functional outcomes for the endoscopic group compared with the EVD group.427,428 One meta-analysis reported higher IVH evacuation rate, lower mortality, improved functional outcomes, and lower permanent shunt rate for endoscopic surgery plus EVD compared with EVD plus IVT.420 No conclusive evidence was provided comparing endoscopic surgery with EVD alone. A network meta-analysis reported improved survival and functional outcomes for endoscopic surgery compared with EVD plus alteplase or urokinase, all of which were superior to EVD alone.419 Lower rates of permanent shunting, intracranial rebleeding, or infection in the endoscopic surgery group suggest that this intervention seems safe, although no large high-quality RCTs directly comparing these interventions have been performed and risk of publication bias is high.
Knowledge Gaps and Future Research
- Current evidence does not support specific recommendations for selecting patients with IVH for EVD in terms of timing or volume of IVH; EVD insertion rates vary widely between hospitals and regions. One retrospective analysis found that small IVH volume (Graeb score ≤2) not associated with obstructive hydrocephalus was not associated with unfavorable outcome or death after ICH, whereas a Graeb score >2 was independently associated with unfavorable outcome and higher mortality.
- Exploratory analyses of CLEAR III suggest associations of improved functional outcome in alteplase-treated patients with larger IVH volumes and randomized earlier after symptom onset. A priori analyses focusing on clinical details (IVH volume and time to initiation of thrombolytic treatment) would inform future recommendations.
- RCTs of IVT and endoscopy have not addressed a priori questions about adequate removal of IVH and optimal timing of the intervention. Further research is needed to determine functional outcome benefit of near-complete IVH evacuation compared with targeting opening of the lower ventricular system and resolution of hydrocephalus and intracranial hypertension.
- Currently, no adequately powered clinical trial data compare different surgical approaches for evacuation of IVH. Are endoscopic techniques superior to EVD plus IVT, and is addition of lumbar drainage superior to EVD alone plus IVT for outcomes or avoidance of permanent shunting?
6.1.3. Craniotomy for Supratentorial Hemorrhage
Referenced studies that support recommendations are summarized in Data Supplements 63 and 64.
Synopsis
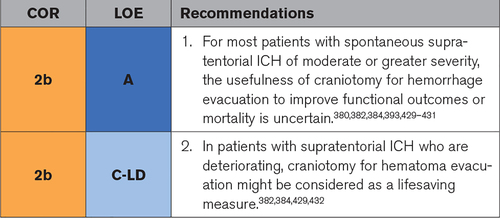
For most patients, craniotomy for spontaneous ICH remains of uncertain benefit compared with medical management alone.429,431 RCT results have been inconclusive. Early data were mixed,393,433–440 with 2 large RCTs finding no benefit in functional outcome or mortality.429,431 However, the most recent of these large RCTs identified a trend toward a mortality benefit, despite a substantial medical-to-surgical crossover rate. In addition, a recent smaller single-center RCT demonstrated a mortality benefit.432 Therefore, limited data suggest that it is reasonable to consider craniotomy as lifesaving procedure in deteriorating patients. A knowledge gap exists concerning the timing of craniotomy for ICH. A small single-arm series of 11 patients raised concern about the safety of craniotomy within <4 hours of onset,436 and STICH (Surgical Trial in Intracerebral Haemorrhage) I and II showed increasing likelihood of achieving a good outcome within a broad therapeutic time window, although surgery was performed primarily >12 hours after onset.441 Two smaller single-center RCTs requiring surgery within ≤12 hours of onset have suggested benefit.430,437 Given these data, further research is indicated to identify whether early (<12 hours) intervention might provide benefit.
Recommendation-Specific Supportive Text
- Craniotomy for ICH of volume >10 mL in patients with significant neurological deficit remains of uncertain benefit compared with conservative management. Both STICH I and STICH II demonstrated no benefit in functional outcome with craniotomy in situations in which the treating neurosurgeon was uncertain about the benefits of either treatment.429,431 A patient-level data meta-analysis performed contemporaneously suggested that certain cohorts might benefit,393 and a smaller (n=108) single-center RCT found that craniotomy improved functional outcome.430 Three meta-analyses published in 2020 provide mixed results: 2 meta-analyses suggest a benefit in functional outcome and mortality with any surgery,382,384 and 1 meta-analysis found no benefit in functional outcome or mortality.380
- Despite the unclear value of craniotomy to improve overall functional benefit or mortality, limited data suggest that craniotomy for hematoma evacuation might be considered as a lifesaving measure in patients who are deteriorating. STICH II found a trend toward improved mortality with surgery, despite a 21% crossover rate from medical therapy to surgery, 74% of which were attributable to deterioration.429 Individuals who crossed over had deeper coma with worse neurological deficits than those in the early surgery group and had worse prognosis compared with individuals who did not cross over, but their surgery did not affect trial results, which were analyzed by intention to treat.429 This suggestion of a mortality benefit was further supported by a recent small (n=61) RCT that demonstrated improved mortality with surgery432 and 2 meta-analyses that suggest a possible mortality benefit.382,384 Therefore, given the crossover attributable to deterioration observed in STICH II and the data suggesting a possible mortality benefit, for patients who are deteriorating, craniotomy for hematoma evacuation may be considered as a life-saving measure.
Knowledge Gaps and Future Research
- The potential impact of timing of craniotomy for ICH on outcome remains debated. Although STICH I and II did not identify an early time effect, a significant majority of enrolled patients underwent surgery >12 hours from onset, and those with surgery <12 hours from onset were likely secondary to severe presentation or deteriorating status. A late time threshold, however, was identified in the STICH I and II cohorts, with expectations of worse outcome beyond 62 hours. Only 2 single-center RCTs have been performed that required surgery within ≤12 hours from onset. The study by Morgenstern et al,437 although not powered for efficacy (n=34), found a promising mortality signal when surgery was performed within 12 hours. More encouragingly, Pantazis et al430 (n=108) demonstrated a benefit in functional outcome when surgery was undertaken within <8 hours. Future multicenter research evaluating the benefit of surgery within 12 hours may clarify this knowledge gap.
6.1.4. Craniotomy for Posterior Fossa Hemorrhage
Referenced studies that support recommendations are summarized in Data Supplement 65.
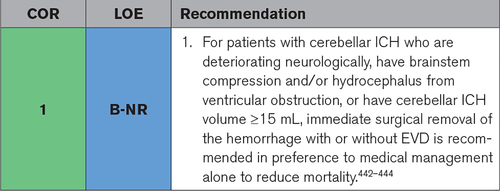
Synopsis
Spontaneous cerebellar hemorrhage is frequently associated with hydrocephalus, brainstem compression, and herniation in the confined space of the posterior fossa.126 Therefore, hematoma evacuation is often recommended despite a lack of randomized evidence.414 The present guideline is based primarily on data from a large individual-patient data meta-analysis with propensity score matching,442 systematic reviews443,444 and several retrospective studies.254,445–451 As a primary recommendation, urgent surgical hematoma evacuation with or without EVD is recommended compared with conservative management to reduce mortality in patients with cerebellar ICH who are deteriorating neurologically, have brainstem compression and/or hydrocephalus from ventricular obstruction, or have cerebellar ICH volume ≥15 mL. The efficacy of surgical evacuation for improving functional outcomes, however, is uncertain and has not been demonstrated in retrospective studies.442 For patients with cerebellar ICH and clinical hydrocephalus, EVD alone is, in theory, potentially harmful, especially if the basal cisterns are compressed.452 EVD alone may be insufficient when intracranial hypertension impedes blood supply to the brainstem.445
Recommendation-Specific Supportive Text
- In an individual-patient data meta-analysis, for patients with spontaneous cerebellar hemorrhage without brainstem extension, hematoma evacuation was not significantly associated with improved functional outcomes at 3 months but was associated with survival benefit at both 3 and 12 months.442 Mortality benefit occurred for patients with larger hematoma volumes (>15 mL), whereas volumes <12 mL were associated with lower likelihood of good outcome with surgery. A systematic review of 41 studies (37 retrospective and 4 prospective) reported no significant association of surgical evacuation with either mortality or functional outcomes at 6 months but, because of a large proportion of retrospective studies, suffered from a high risk of bias.443 A large retrospective review found that pooled mortality rates were lower in patients treated with surgery compared with conservative treatment but functional outcomes were more favorable with nonsurgical management.444 This may reflect variable indications for surgery. Another study reported mortality reduction with surgery in cases with hydrocephalus, but not without, indicating the importance of treating hydrocephalus.450 One retrospective study reported trends for improved mortality and functional outcome for suboccipital decompression and hematoma evacuation compared with evacuation alone.448 Most studies support a lifesaving benefit from surgery under conditions of a deteriorating clinical examination, impending brainstem compression, clinical hydrocephalus with fourth ventricle obstruction, and radiographic obliteration of basal cisterns.442,445–448,450,451
Knowledge Gaps and Future Research
- A perceived lack of equipoise concerning the lifesaving benefits of surgical evacuation for cerebellar ICH most likely precludes the design of future randomized trials to address the question of surgical versus conservative management. The efficacy of surgical evacuation for improving functional outcomes remains uncertain.
- Previous studies have not addressed a priori questions about timing of surgery for cerebellar ICH and specifically whether initial conservative treatment compared with immediate surgical evacuation is preferable in patients with cerebellar ICH >3 cm/15 mL who are in a good clinical condition. For such patients, a retrospective study reported that an initial conservative approach often leads to good outcome and that there may be a subgroup of patients in whom surgery can be safely deferred. The optimal timing and indications of surgical treatment in large cerebellar ICH with good clinical condition are worthy of further study.
- Currently, no adequately powered studies have compared different surgical approaches for cerebellar ICH. Several small retrospective studies compared endoscopic evacuation or stereotactic aspiration with standard suboccipital craniectomy, with variable efficacy. Comparison of MIS techniques with suboccipital hematoma evacuation with or without decompression is an important topic for future clinical trials. Further investigation also is needed to determine whether MIS in patients with >15-mL cerebellar ICH volume and good clinical condition improves functional outcome compared with best medical treatment.
Referenced studies that support recommendations are summarized in Data Supplements 66 through 68.
Synopsis
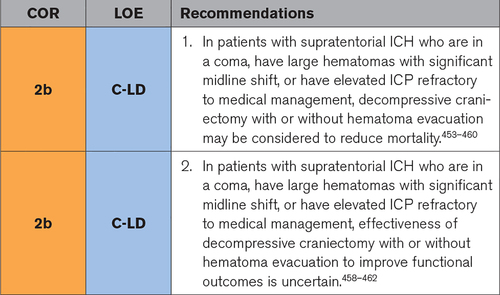
Large supratentorial ICH is often associated with clinical deterioration and elevated ICP that is refractory to medical management. Therefore, decompressive craniectomy is often considered as a lifesaving procedure despite a lack of strong randomized evidence. This guideline is based primarily on data from small RCTs,458,462 retrospective series,453–457,461,463–471 a systematic review,459 and a meta-analysis.460 These studies compared decompressive craniectomy with medical management or craniotomy with clot evacuation. Reports also compared decompressive craniectomy alone with decompressive craniectomy with clot evacuation. As a primary recommendation, decompressive hemicraniectomy may be considered to reduce mortality in patients with supratentorial ICH who are in a coma, have large hematomas with midline shift, or have elevated ICP refractory to medical management. No clear differences have been demonstrated between decompressive hemicraniectomy with and without clot evacuation.461 The efficacy of decompressive craniectomy for improving functional outcomes is uncertain.
Recommendation-Specific Supportive Text
- Retrospective case series demonstrate that decompressive craniectomy is safe and feasible. The majority of studies examine patients in a coma (GCS score <8), with hematomas >30 mL, or with ICP that did not normalize with medical management.454,458,462,463,465,466,468,471 Many include patients within 24 hours of hemorrhage. Overall, the studies suggest that surgery may improve mortality compared with medical management.453–457,470 Both a meta-analysis and a systematic review suggest that decompressive craniectomy may offer mortality benefits in the setting of supratentorial ICH.459,460 Studies included in these analyses compare decompressive craniectomy with both medical management and craniotomy with clot evacuation. The systematic review (1 RCT, 8 retrospective studies) included only patients who underwent decompressive craniectomy without clot evacuation and reported a mortality rate of 26%.459
- There is less evidence of beneficial effects of decompressive craniectomy on functional outcome than on mortality. One RCT assessed decompressive craniectomy without hematoma evacuation against hematoma evacuation without decompressive craniectomy in deep supratentorial ICH.462 This study found no difference in mortality at 6 months and slightly higher GCS score (improved outcome) for patients undergoing hematoma evacuation alone (35.3%) compared with decompressive craniectomy alone (30.7%). Another RCT assessed adding decompressive craniectomy and expansive duraplasty to hematoma evacuation versus hematoma evacuation alone for large hypertensive ICH.458 This study demonstrated reduced mortality (10% versus 25%) and improved functional outcome (70% versus 20% with favorable outcome) at 6 months in the decompressive craniectomy plus expansive duraplasty cohort.458 Retrospective case series that compare decompressive craniectomy and craniotomy with hematoma evacuation present conflicting results (some favor decompressive craniectomy, others favor hematoma evacuation).463–469 A single retrospective study compared decompressive craniectomy with and without associated hematoma evacuation. Performance of hematoma evacuation did not change functional outcomes.461 A meta-analysis (1 RCT, 7 observational studies) reported that decompressive craniectomy significantly reduced poor outcome compared with the control group, but only for studies using hematoma evacuation as control.460 The systematic review reported a pooled favorable outcome in 53%.459
Knowledge Gaps and Future Research
- There is a perceived lack of equipoise regarding the lifesaving benefits of decompressive craniectomy for supratentorial ICH and medical management. The efficacy of surgical evacuation for improving functional outcomes, however, remains uncertain. The currently enrolling SWITCH trial (Decompressive Hemicraniectomy in Intracerebral Hemorrhage) will investigate these questions (ClinicalTrials.gov NCT02258919).
- Previous studies have not directly addressed timing of decompressive craniectomy surgery in the setting of ICH. It is unclear whether the benefits of surgery would be greater within a specific time window. Future studies could help determine the optimal timing of decompressive craniectomy in large supratentorial ICH.
- There is also limited guidance from the literature on appropriate patient selection for decompressive craniectomy. For example, it is not known how patient-specific factors such as age, degree of language involvement, and medical comorbidities may influence mortality and functional outcomes after decompressive craniectomy for supratentorial ICH.
- The ideal decompressive craniectomy size has not been studied in patients with ICH. However, literature exists with respect to hemicraniectomy size in the setting of ischemic stroke, head trauma, and subarachnoid hemorrhage. Future studies in patients with ICH could help determine the optimal size of craniectomy flap and the effects that the size of the hemicraniectomy has on ICP measurements and patient outcome.
8. Post-ICH Recovery, Rehabilitation, and Complications
8.1. Rehabilitation and Recovery
Referenced studies that support recommendations are summarized in Data Supplement 71.
Synopsis
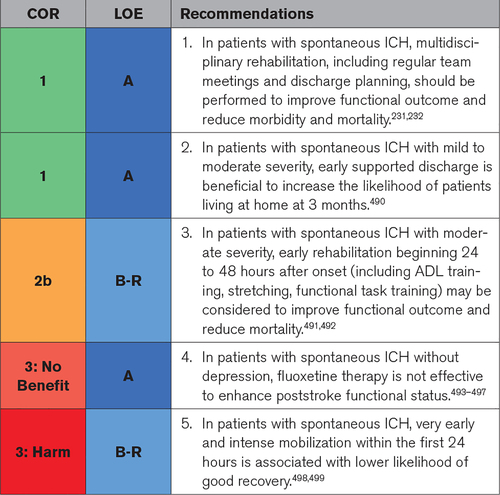
Stroke rehabilitation includes a number of tailored measures from different professionals with different intensity that depends on individual patient needs and time since stroke. The outcome of rehabilitation is thought to be a combination of recovery attributable to reorganization in the brain and compensatory strategies. To improve multidisciplinary teamwork on the ward, weekly team meetings to discuss patient discharge and appropriate timing are important and improve functional outcome. Starting rehabilitation after 24 to 48 hours after stroke onset seems beneficial; however, intense and frequent mobilization within the first 24 hours is not recommended. Early supported discharge allows care and services to be transferred from the hospital to the home (community setting) and improves the likelihood for independent living. Brain plasticity is the ability of neural networks in the brain to alter through expansion and reorganization, and fluoxetine has been tried in animals with promising results. However, in patients after stroke, it does not improve recovery. We note that much of the data on recovery and rehabilitation come from studies of all types of stroke and mention data from ICH subgroups when available.
Recommendation-Specific Supportive Text
- Stroke unit care is a model in which a multidisciplinary team of stroke specialists looks after patients with stroke in hospital. The components include500 structured assessment procedures, coordinated multidisciplinary team care with regular meetings (at least weekly in many of the studies, although the optimal timing has not been defined), and early assessment for planned discharge. This leads to improved functional outcome and reduces mortality independently of patient age, sex, initial stroke severity, and stroke type.232
- Many patients with mild to moderate disability (eg, mRS score ≤3) after ICH can benefit from early supported discharge.490 This allows patients to continue their rehabilitation therapy at home, with intensity and expertise similar to that of the rehabilitation they would receive in hospital. Early supported discharge not only reduces hospital time but also increases the likelihood that the patient will continue living at home independently compared with those who have had their rehabilitation as inpatients. Early supported discharge also improved the patient-therapist partnership and motivated patients by focusing on realistic rehabilitation goals in the more relevant context of home living and management. This has been shown to work in different countries with different health care systems (Sweden,501 Canada,502 Australia,503 Norway,504 Thailand,505 Northern Ireland506).
- Studies generally support early institution of rehabilitation activities. In a Chinese study492 that compared early rehabilitation as an add-on to usual care, family members were instructed to perform basic rehabilitation (exercises of daily living, stretching exercises, neuromuscular electric stimulation, and functional training such as grasping and pointing) starting within 48 hours of ICH. The study randomized 243 patients (excluding those with either severe or minor deficits) and showed that the intervention resulted in improved survival and functional outcome at 6 months. A multicenter, international study491 with >11 000 patients with acute stroke (15% ICH) compared lying-flat position to a sitting-up position with the head elevated to at least 30° for the first 24 hours. Lying flat to improve cerebral perfusion was not associated with benefit for the primary outcome, mRS score at 90 days.
- The concept of enhancing brain plasticity through use of selective serotonin reuptake inhibitors (SSRIs) has been suggested by animal model studies.495 However, multiple studies of fluoxetine, in either patients with ICH or patients with stroke in general, have not shown beneficial effects on functional outcome.493–497 Patients allocated fluoxetine were less likely to develop new depression by 6 months than patients on placebo but were more prone to fractures.
- A trial of very early mobilization (AVERT [A Very Early Rehabilitation Trial) compared frequent, higher-dose, and very early mobilization with usual care in 2104 patients with stroke, of whom 258 (12%) had ICH.499 The intervention was defined as a standardized treatment beginning within 24 hours of stroke onset, focusing on sitting, standing, and walking and resulting in at least 3 additional out-of-bed sessions compared with usual care (increase intensity). The study included >2100 patients in 5 countries and showed that the intervention increased the risk of poor outcome at 3 months. A prespecified subanalysis in patients with ICH showed that this early and intense intervention led to an increased risk of mortality at 14 days after stroke.498
Knowledge Gaps and Future Research
- An area for future study is patients’ return to work, driving, and participation in other meaningful social activities. The current literature in this area is based largely on epidemiological studies. Greater independence in ADLs, fewer neurological deficits, and better cognitive ability were the most common predictors of return to work. More studies are needed to investigate how vocational rehabilitation should be performed and the role of occupational/vocational therapy in this process.
- There is a knowledge gap from the professionals’ side concerning sexual life after ICH, contributing to the infrequency of this topic being addressed in the conversation with patients. Many people fear returning to sexual activity after stroke. However, it seems as though intercourse increases BP only slightly (up to ≈140 mm Hg) for a short time, and then it recovers to baseline level soon after sexual activity in healthy adults.
- There is a lack of knowledge about physical training after ICH. For example, it is unclear how to guide people after ICH in terms of weight lifting (lifts using large muscle groups versus small, heavy lifts versus repetitive lifts) and how much and how long to raise their BP. Furthermore, it is unclear what to advise about any potential bleeding risk related to exertion when BP gets >300 mm Hg.
- There are insufficient data on medications to improve post-ICH functional outcome. Neurostimulants, for example, have not been studied extensively for recovery of consciousness or other recovery steps after ICH.
- Another emerging recovery modality that should be studied after ICH is remote video administration of rehabilitation activities (telerehabilitation).
8.2. Neurobehavioral Complications
Referenced studies that support recommendations are summarized in Data Supplements 72 and 73.
Synopsis
Mood disturbances and cognitive dysfunction are common consequences after ICH. Poststroke depression occurs in 20% to 25% of patients with ICH within the first year after stroke,522 and this persists over time.523 Thirty-three percent of patients with ICH experience dementia either before or after their ICH,524 and the incidence of post-ICH dementia increases over time, with 1 study showing an incidence of new-onset dementia of 14.2% at 1 year, increasing to 28.3% at 4 years.525 Another study noted 32% prevalence of cognitive impairment at 3 years after stroke.526 Analysis of neuroimaging features of patients who develop post-ICH dementia suggests underlying CAA as a contributing factor.525 Neurobehavioral complications after ICH are underrecognized by clinicians, leading to worsened long-term patient-centered outcomes such as independence and community reintegration.527 Poststroke depression is associated with increased short- and long-term mortality528–532 and poor functional outcomes532–534 and leads to greater physical limitations, which can impair rehabilitative efforts.535 Poststroke depression also can lead to suicide, which is twice as high in the first 2 years after stroke compared with the general population.536 Similarly, cognitive impairment predicts poststroke disability526,535,537 and mortality.537–539 There is also an interaction between the two: Cognitive symptoms can be caused by depression, and depression can interfere with cognitive function. Recognition and treatment of these stroke complications can have a large impact on stroke recovery.
Recommendation-Specific Supportive Text
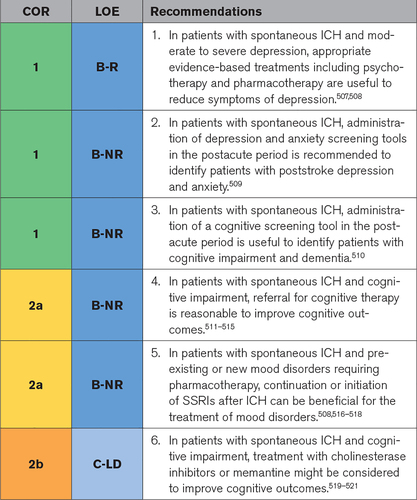
- Patients with poststroke depression and anxiety should be referred to a mental health professional for consideration of psychotherapy or talking-based therapy because several meta-analyses have shown a significant improvement in depression scores540,541 and remission of poststroke depression540,541 in patients who underwent psychotherapy with or without pharmacotherapy. Psychotherapy also significantly reduces poststroke anxiety.542 Pharmacological therapy is beneficial in reducing poststroke depression and anxiety prevalence and symptoms.540,542–548 Three of the randomized trials evaluating fluoxetine for motor recovery after stroke showed reductions in poststroke depression when fluoxetine was started 2 to 15 days after ischemic stroke or hemorrhagic stroke.493,496,549 Several studies suggest that transcranial magnetic stimulation also reduces symptoms of poststroke depression.544,550
- Validated screening tools to evaluate for depression and anxiety can lead to improved patient outcomes. One prospective RCT found a significant improvement in depression symptoms for patients with acute ischemic stroke when screening was paired with an Activate-Initiate-Monitor intervention, where Activate represents patient recognition of depression‚ Initiate represents antidepressant medication‚ and Monitor represents treatment.551 In a meta-analysis, Meader and colleagues509 evaluated the Center for Epidemiological Studies Depression Scale, Hamilton Depression Rating Scale, and Patient Health Questionnaire-9. All had optimal receiver-operating characteristics curves to detect poststroke depression and anxiety. Therefore, any of these screening tools can be used to assess for post-ICH mood disorders. Although many studies report poststroke depression during hospitalization and rehabilitation, mood disorders recur over time. For patients who developed poststroke depression, recurrence increased from 28% in year 2 to 100% by year 15.529 Although the optimal timing and frequency of depression screening are uncertain, screening should occur not only at transition points across the continuum of care (eg, hospitalization to inpatient rehabilitation) but also in the outpatient setting, especially for patients with a history of poststroke depression within the first year after ICH.529
- Multiple tests are available to screen for cognitive impairment. A meta-analysis compared studies evaluating the Mini-Mental State Examination, Montreal Cognitive Assessment, Rotterdam–Cambridge Cognition Examination, and Addenbrooke’s Cognitive Examination–Revised and showed that all demonstrated similar accuracy to detect cognitive impairment and dementia.510 The Montreal Cognitive Assessment has a high specificity and was shown in 1 study to be the most valid and clinically feasible tool across a wide range of cognitive impairment,507 but it has a lower specificity for screening.510,552 The Depression, Obstructive Sleep Apnea, and Cognitive Impairment screening tool takes <5 minutes to administer and may be more practical for assessment of multiple conditions in an outpatient clinic appointment.527,553 Because there is no superior screening test, consideration should be given to feasibility and level of concern for cognitive impairment in the selection of a particular test. Timing of initial screening is uncertain. Delirium often confounds cognitive assessment during inpatient admission but is associated with posthospital cognitive impairment and reduced quality of life.554,555 The patient’s family and caregivers should be included in the assessment. Evidence shows that dementia continues to develop after ICH; thus, screening should occur across the continuum of inpatient care and at intervals in the outpatient setting. Although detection of post-ICH cognitive impairment is likely to be useful information for the patient’s family and care team, it should be noted that current treatments for cognitive impairment appear to have no more than modest benefits.
- Cognitive therapy, broadly defined as standardized tasks designed to engage, maintain, and improve a patient’s thinking skills, has shown mild to modest benefits in improving overall cognitive function for patients with dementia in multiple meta-analyses.511,515,556,557 The quality of evidence in these studies is hampered by heterogeneity in the types and length of treatment and severity of dementia and a lack of standardization of rehabilitative interventions. In patients with stroke with dementia, the benefits of cognitive therapy have been less clear, with meta-analyses showing uncertain benefits in improvement of attention deficits,513 memory deficits,514 and executive dysfunction.512 The potential benefits of cognitive therapy for post-ICH dementia have not been well established, but given the potential benefits based on a generalized dementia population and lack of side effects, it is reasonable to refer patients with ICH with cognitive impairment or dementia for cognitive therapy.
- The use of SSRIs is beneficial to reduce symptoms of depression and anxiety after stroke.508,558 Specific caution should be used when initiation of SSRI therapy in an ICH population is considered. Several meta-analyses have shown a small but increased risk of ICH with the use of SSRIs,508,516,517,559 especially in patients who are taking anticoagulation and strong SSRIs.508,559,560 This can translate into worsened 3-month neurological outcome.518 Conversely, 4 randomized trials that evaluated the use of fluoxetine for stroke motor recovery did not show an increased risk of hemorrhagic stroke compared with placebo.493,494,496,536,549 In patients with ICH, SSRIs should therefore be reserved for patients with moderate to severe depression to balance the importance of treating depression with the risk of increased hemorrhage.
- There have been no specific trials of treatment of ICH-related cognitive impairment and dementia, but pharmacological therapy has been shown to be beneficial in other types of dementia and cognitive impairment. In the most recent Cochrane reviews, use of memantine has shown a beneficial effect on cognitive function, ADLs, and mood in patients with moderate to severe Alzheimer disease and an improvement in cognitive function, behavior, and mood in mild to moderate vascular dementia,521 with side effects such as headaches and dizziness. The cholinesterase inhibitor donepezil has been shown more consistently to improve cognitive function and ADLs in patients with vascular cognitive impairment and all levels of Alzheimer dementia,519,520 with significant side effects such as nausea, diarrhea, anorexia, and cramps. Therefore, it may be reasonable to consider using cholinesterase inhibitors for mild to moderate dementia and memantine for moderate to severe dementia after ICH.
Knowledge Gaps and Future Research
- Further research is needed to determine the optimal screening tools, timing, and frequency of screening for post-ICH depression, anxiety (generally less studied than depression), and cognitive impairment. Given concerns that screening can take time in a busy outpatient practice, rapid screening tools should be developed and validated to ensure identification of these important neurobehavioral consequences of ICH.
- There is a paucity of data on risk of ICH for specific SSRI medications or distinguishing risk profiles between SSRIs and other antidepressant classes such as serotonin-norepinephrine reuptake inhibitors, leading to uncertainty about individual medication choices in patients with ICH who require pharmacotherapy for the treatment of depression. The relative risks and benefits of SSRI or serotonin-norepinephrine reuptake inhibitor use in the ICH survivor population with depression require further prospective evaluation.
- It is unclear whether the same pharmacological agents used to treat Alzheimer dementia, vascular dementia, and cognitive impairment are beneficial to treat post-ICH cognitive impairment. This is an area of future research.
9. Prevention
9.1. Secondary Prevention
9.1.1. Prognostication of Future ICH Risk
Referenced studies that support recommendations are summarized in Data Supplement 74.
Synopsis
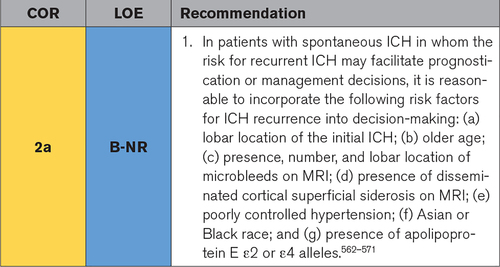
Survivors of ICH are at risk for hemorrhage recurrence. The estimated recurrence risk ranges from 1.2%/y to 3%/y across undifferentiated patients with ICH, with the highest event rate in the first year after the incident hemorrhage.562,565–571 However, the individual risk of recurrence can vary considerably according to the underlying pathogenesis (resulting from the higher recurrence rates for ICH associated with CAA relative to arteriolosclerosis), demography, and overall clinical context. A pooled analysis of 325 individuals with ICH diagnosed as attributable to CAA found a recurrence risk of 7.4%/y (95% CI, 3.2%/y–12.6%/y), substantially greater than in the 981 individuals diagnosed with non–CAA-related ICH (recurrence rate, 1.1% [95% CI, 0.5%–1.7%]).564 Clinical assessment and laboratory testing, including MRI, are helpful for recurrent ICH risk stratification and optimal overall vascular management. A careful assessment of individual recurrence risk may be warranted because patients with ICH are also at risk of ischemic stroke and other major vascular events.571 In such scenarios, antithrombotic medications are often contemplated, and the risk of hemorrhage must be weighed against the risk of ischemic and vaso-occlusive disease. (The complex decision-making process for incorporating this information is addressed in Section 9.1.3, Management of Antithrombotic Agents.)
Recommendation-Specific Supportive Text
- Radiological features suggestive of underlying amyloid angiopathy are associated with the highest risk of ICH recurrence. These include a prior lobar ICH (HR, 4.8),572 the presence of microbleeds27,573,574 (in particular strictly lobar microbleeds),27,575 the number of lobar microbleeds (HR, 1.88 for 1 microbleed, 2.93 for 2–4 microbleeds, 4.12 for >4 microbleeds),572 and the presence of disseminated cortical siderosis (HR, 4.69).576,577 The presence of microbleeds and cortical siderosis can be determined during the etiological workup of ICH (Section 4.1, Diagnostic Assessment of Acute ICH Course). Carriers of apolipoprotein E genotypes associated with amyloid angiopathy are similarly at higher risk of ICH recurrence compared with those with the more common ε3/ε3 genotype; those with the ε2 or ε4 allele have an HR of 3.3 and 2.5 for recurrence, respectively.578 Recurrence risk also increases with higher measured outpatient BP563 and age570,579 (HR, 2.8 in age >65 years) and is higher in those of Black race (HR, 1.22) or Asian race (HR, 1.29) compared with White race (race defined by self-designation, clinicians, or administrative personnel while in hospital).568 Association of ICH recurrence with Hispanic ethnicity has been inconsistent.568,580
Knowledge Gaps and Future Research
- There is insufficient evidence to estimate ICH recurrence risk on an individual-patient basis. Deriving and validating a prediction rule incorporating clinical, radiological, and genotype biomarkers and determining the most informative thresholds for categorizing these factors would be helpful to estimate the risk of recurrence.
- The mechanism by which race is associated with ICH recurrence, including the likely crucial role of social determinants of health, is unclear. More research into this association is required.
- MRI findings suggestive of small vessel disease may reflect an increased risk for ICH recurrence. More research is needed into the recurrence risks associated with T2 hyperintensities, enlarged perivascular spaces, microangiopathic changes, intragyral hemorrhage, and lobar versus nonlobar microbleeds.
9.1.2. BP Management
Referenced studies that support recommendations are summarized in Data Supplements 75 and 76.
Synopsis
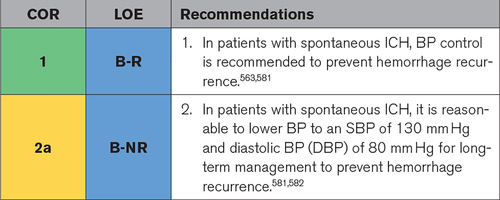
Hypertension has a strong causal association with ICH and is a major modifiable risk factor for all stroke subtypes. Uncontrolled hypertension accounts for 73.6% of the global population-attributable risk for ICH.93 Despite this, a significant proportion of ICH survivors continue to have poorly controlled BP.563,583 Moreover, patients with ICH are also at risk of future ischemic stroke and cardiovascular disease because of overlapping risk factors. Treating hypertension after ICH is a safe and effective way to mitigate future ICH risk and reduce events across the spectrum of vascular disease.581 It is therefore critical to measure and identify uncontrolled hypertension after ICH and aggressively manage BP to prevent recurrence.
Recommendation-Specific Supportive Text
- In a large prospective cohort study of 1145 patients with primary ICH and a median follow-up of 36.8 months, inadequate BP control was associated with increased risk of both lobar (HR, 3.53 [95% CI, 1.65–7.54]) and nonlobar (HR, 4.23 [95% CI, 1.02–17.52]) ICH recurrence.563 In PROGRESS (Perindopril ProtectionAgainst Recurrent Stroke Study), treatment with perindopril and indapamide reduced mean BP by 10.8/4.4 mm Hg in patients enrolled with ICH and resulted in a relative risk reduction of 42% (95% CI, 14–60) in major vascular events and a number needed to treat of 18 to prevent ICH recurrence over 5 years.581 The optimal timing for BP lowering after ICH is not known, and a decision to initiate antihypertensive therapy in the acute setting should be in accordance with the recommendations discussed in Section 5.1, Acute BP Lowering.
- In the PRoFESS trial (Prevention Regimen for Effectively Avoiding Second Strokes), the risk of ICH during follow-up was higher in subjects with SBP ≥160 mm Hg compared with those with SBP of 130 to 139 mm Hg (HR, 2.07 [95% CI, 1.22–3.51]), with a nonsignificant trend toward lower rates of ICH with SBP <130 mm Hg. Similarly, the risk of ICH was higher in subjects with DBP ≥100 mm Hg compared with DBP of 80 to 89 mm Hg (HR 2.58 [95% CI, 1.50–4.45]).582 In a large prospective cohort study of 1145 patients with primary ICH, the risk of ICH recurrence was significantly higher for patients with SBP ≥120 mm Hg and DBP ≥80 mm Hg compared with patients who had SBP <120 mm Hg and DBP <80 mm Hg.581,584 The relationship between SBP and ICH recurrence was continuous with an HR of 1.33 and 1.54 per 10-mm Hg increase for recurrent lobar and nonlobar ICH, respectively. Although a continuous relationship allows some flexibility with specific BP goals, the ICH evidence supports the ≤130/80-mm Hg target recommended in the 2017 hypertension clinical practice guidelines.585
Knowledge Gaps and Future Research
- The ideal target BP to prevent ICH recurrence is not known. More research is required to determine whether a more aggressive target of SBP of ≤120 mm Hg is beneficial.
- The timing to initiate BP therapy and the optimal class of medication to achieve control are uncertain. Moreover, emerging research suggests that home BP measurements may be a more accurate measure of control. The timing of therapy, best choice of antihypertensive medication, and best approach to outpatient BP monitoring require further study.
- It will be important to determine the predominant factors at the individual, systemic, and societal levels that preclude optimal BP control and identify strategies to overcome these barriers.
9.1.3. Management of Antithrombotic Agents
Referenced studies that support recommendations are summarized in Data Supplements 77 through 79.
Synopsis
Antithrombotic therapy is a mainstay of treatment for patients with ischemic cardiovascular or cerebrovascular disease or a history of thromboembolic events. Clinical decision-making concerning the use of antithrombotic medications once these patients have an ICH remains challenging given the paucity of prospective RCTs addressing specific patient populations. Individual patient decisions remain that are based on assessments of risks and benefits of antithrombotic therapies in the context of the published literature of recurrent event rates. Furthermore, data on optimal timing to resume antithrombotic therapy in patients in whom it will be resumed remain sparse. Further discussion of risk factors for recurrent ICH is given in Section 9.1.1, Prognostication of Future ICH Risk. These risks may assist clinicians in patient selection.
Recommendation-Specific Supportive Text
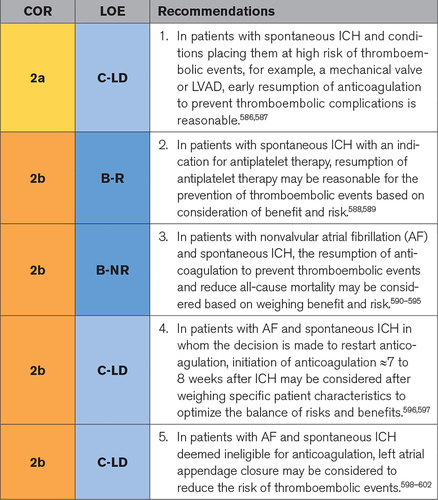
- The balance of prothrombotic risks in patients with ICH and an LVAD or mechanical valves with the recurrent hemorrhagic risk of anticoagulation resumption remains challenging. There are sparse data on the risk and timing of device thrombosis versus worsening hemorrhage, and data remain observational. One study found that in patients with LVAD, anticoagulation resumption with warfarin at a median of 14 days from the index ICH was associated with fewer fatal and nonfatal thrombotic events than the resumption of antiplatelet alone, and there was no significant difference in recurrent ICH rates.586 In an observational study of 22 patients with LVAD with ICH, none had evidence of LVAD thrombosis after reversal and holding of anticoagulation for up to 13 days.182 In patients with mechanical heart valves, 1 study reported that although complications were significantly increased when anticoagulation was resumed before day 14, the composite of hemorrhage and thromboembolic risk suggested that anticoagulation may be considered in those with mechanical valves as early as day 6 from the index ICH.587 The decision to restart anticoagulation (eg, at 14 days after ICH for patients with LVAD and potentially earlier for patients with mechanical valves and relatively small ICHs) is therefore reasonable and safe in patients with LVAD or mechanical valves but requires individualized assessment of risk and benefit.
- The decision to continue antiplatelet therapy in patients with a history of ischemic vascular events who have an incident ICH is challenging given concerns about the risk of ICH recurrence. One open-label RCT addressed this question.589 In 537 patients randomized at a median of 76 days after ICH onset and followed up for a median of 2 years, treatment with antiplatelet medications led to no increased risk of ICH and a reduction in the composite end point of nonfatal myocardial infarction, nonfatal stroke (including ICH and ischemic stroke), and death resulting from a vascular cause. On extended follow-up for up to 7 years, the study found no statistically significant effect of antiplatelet therapy on recurrent ICH or all other major vascular events.603 These results are consistent with a large meta-analysis of 1916 patients with ICH that reported no significant increase in risk of ICH recurrence and a decreased risk of thromboembolic and ischemic events with resumption of antiplatelet therapy.588 Important caveats include a scarcity of data on risk differences by location or cause of ICH, lack of blinding, and selection bias in patient enrollment based on clinician assessments of risk. Individual clinician assessment of patients’ risks of recurrent ICH and benefits of antiplatelet therapy is needed, but the available data support that, in appropriate patients, the resumption of antiplatelet therapy is reasonable. The optimal timing for resuming antiplatelet therapy has not been systematically studied.
- A number of retrospective analyses have attempted to address the risks and benefits of anticoagulation therapy in patients with both nonvalvular AF and a history of ICH.179,590,591,593–595,604 The studies vary by design, including national registries and retrospective and prospective cohorts; have variable inclusion and exclusion criteria and timing to the initiation of anticoagulation; generally study VKA therapy; and include some replication of cohorts across studies. With these limitations, which include systematic differences between anticoagulated and nonanticoagulated individuals attributable to the confounding of choice of therapy by clinician-perceived risk-benefit profile, the published literature suggests a potential reduction in recurrent ischemic events and all-cause mortality with the use of anticoagulation. Anticoagulation may be considered in select patients‚ based on assessments of risk and benefit, and enrollment in ongoing prospective RCTs should be prioritized to address this clinical dilemma. Given the reduced risk of ICH with DOACs compared with VKAs in stroke prevention trials and real-world practice, these may be favored in patients with a history of ICH if anticoagulation is deemed indicated, although data are lacking.
- The timing of resumption or initiation of anticoagulation in patients with AF and ICH remains challenging. A study suggests that a composite net benefit of stroke risk reduction and bleeding risk minimization occurs when anticoagulation is started 7 to 8 weeks after ICH.597 Before 4 to 8 weeks, there appears to be a significant increase in bleeding risk.596,597 These studies suggest that the optimal timing of initiation of anticoagulation is ≈8 weeks after the index ICH. However, these studies are limited by confounding by indication and clinician and patient preferences. Therefore, timing should be considered on a case-by-case basis of individual risk assessments of thromboembolism, recurrent ICH, and late ICH expansion.
- Left atrial appendage closure is an alternative in patients with AF and ICH who have contraindications to long-term oral anticoagulation. Two meta-analyses of the PROTECT-AF trial (WATCHMAN Left Atrial Appendage System for Embolic Protection in Patients With Atrial Fibrillation) and PREVAIL trial (Evaluation of the WATCHMAN Left Atrial Appendage [LAA] Closure Device in Patients With Atrial Fibrillation Versus Long Term Warfarin Therapy) reported outcomes in patients randomized to left atrial appendage closure or warfarin therapy.598,599 Rates of ischemic stroke with left atrial appendage closure did not demonstrate noninferiority compared with warfarin, but rates of hemorrhagic stroke and bleeding were lower, and the primary end point of stroke, systemic embolism, and cardiovascular death was similar across the 2 treatment arms.598,599 In patients with a history of ICH and AF, data from a small, nonrandomized, retrospective cohort showed lower cardiovascular mortality, all-cause mortality, hemorrhagic stroke risk, and major bleeding events with left atrial appendage closure compared with standard medical therapy.601 Other small retrospective studies reported low event rates similar to rates in the patients without ICH600 and no ischemic stroke or ICH within 30 days of left atrial appendage closure among patients diagnosed with CAA.602 Application of these results to individual patients with ICH remains unclear because of the potential confounding by patient selection, limited numbers of patients reported, and lack of standardization of time interval to left atrial appendage closure, type of antiplatelet or anticoagulant, and duration of treatment before and after implantation.
Knowledge Gaps and Future Research
- In addition to the uncertainty of risk and benefit of anticoagulation in patients with AF and ICH, there is limited evidence for individual selection of optimal timing of anticoagulation resumption in patients for whom anticoagulation will be restarted. Ongoing trials and future studies with stratification based on ICH location, mechanism, and risk factors for recurrence may lead to more informative decisions.
- Most analyses evaluating the role of appropriate antithrombotic therapy in patients with ICH have focused on recurrent events. Future studies that incorporate outcomes such as disability or quality of life in addition to clinical events may provide information that is more patient-centric. More research is also needed on the timing of resumption of antiplatelet therapy and the differences in benefits and risks among different agents by different indications and across sex, racial, and ethnic groups.
- Prospective data are lacking on the safety and efficacy of left atrial appendage closure in patients with ICH, particularly when performed within 6 months from the index ICH. This is important given that most patients under consideration for device implantation are under a time-sensitive risk-benefit analysis based on thromboembolic risk of untreated AF. Future studies may need to explore earlier timing and better standardized type and duration of antiplatelet therapy or anticoagulation therapy before and after implantation. As for all device-related therapies, future changes in left atrial appendage closure device type may affect patient outcome.
9.1.4. Management of Other Medications
Referenced studies that support recommendations are summarized in Data Supplements 80 and 81.
Synopsis
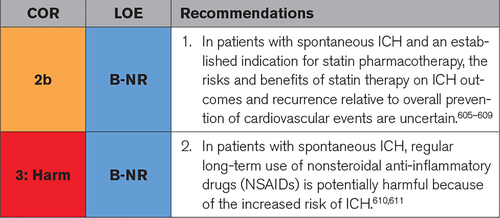
Several classes of medications, including SSRIs, statins, and NSAIDs, have the potential for increased risk of recurrent ICH, raising the clinical dilemmas of medication management in patients taking these medications who have an incident ICH. Statin therapy in patients with ICH was associated with an increased risk of recurrent ICH in the SPARCL trial (Stroke Prevention by Aggressive Reduction in Cholesterol Levels).606,612 However, other observational, nonrandomized studies have not found this association in patients with hypercholesterolemia, and risk may depend on the patient risk for recurrent ICH and type of statin used.607,609,613–618 For both classes of medications, the indications and risk-benefit profiles for an individual patient must be weighed. NSAID use is associated with an increased risk of bleeding610,611; thus, regular long-term use should be avoided when possible in patients with ICH. (SSRI use is discussed in Section 8.2, Neurobehavioral Complications.)
Recommendation-Specific Supportive Text
- The association of statin use with both acute outcomes and the reduction of recurrent vascular events in patients who have had an ICH has been uncertain. The SPARCL study identified an increased risk of ICH with high-dose atorvastatin use in the setting of very-low-density lipoprotein levels.612 Post hoc analyses identified entry into the trial with an ICH as the stroke subtype conveying the highest risk for subsequent ICH but did not find an association between ICH and the most recent pre-ICH low-density lipoprotein value.606 Additional nonrandomized, observational studies have not found an association with statin use in patients with ICH.607,609,613,616,618 The risk may be mediated by complex interactions among genetic risk of recurrent ICH, lipid levels, and ICH location.614,617 In addition, lipophilic statins may be associated with higher rates of ICH than hydrophilic statins.615 Other retrospective analyses suggest the potential for improved outcomes after ICH with statin use605,619,620 and a reduction in short- and long-term mortality with statin use.608,618,621–627 However, the results should be interpreted with caution because of selection bias and confounding by indication in these nonrandomized studies. Given this uncertainty, the decision to use statins in patients with ICH depends on risk assessment of ischemic cardiovascular and cerebrovascular events versus recurrent ICH. Enrollment in ongoing randomized clinical trials addressing this question can be encouraged. Clinical trials of the lipid-lowering PCSK9i (proprotein convertase subtilisin/kexin type 9 inhibitors) have thus far not suggested increased risk of first ICH but have not yet examined risk of recurrence in patients with prior ICH.628–630
- The use of NSAIDs is associated with an increased risk of bleeding. Overall event rates of ICH are low in the general population, but a large meta-analysis of observational studies found an increased risk of hemorrhagic stroke with diclofenac and meloxicam use.611 A subsequent large meta-analysis found an increased risk of ICH with any NSAID use.610 One small study of patients with ICH with short-term outcomes found no association of NSAID use with outcomes and recurrent ICH, but follow-up was limited to 90 days.631 Given the increased risk of bleeding with NSAID use, that patients with ICH are at higher risk of recurrent ICH than the general population, and the existence of safer alternatives to NSAID such as acetaminophen for most indications, the regular (eg, daily) use of NSAIDs after an ICH is not recommended, although randomized data and data drawn from individuals with ICH are lacking.
Knowledge Gaps and Future Research
- The effect of statins on long-term incident ischemic and hemorrhagic events in patients with ICH is uncertain, as is the effect of statin use on short-term outcomes after ICH. Ongoing and future studies to identify patient populations who may benefit from both short- and long-term statin use or from changing to an alternative lipid-lowering agent such as ezetimibe or a PCSK9i are needed.
- Further research on radiological and biological markers that may further refine risk of recurrence such as MRI markers of cerebral small vessel disease, genetic risk, BP, and medication interactions would aid in the risk stratification in patients requiring the use of these medications.
- There is growing but still uncertain evidence that some commonly used medications other than the antithrombotics may increase ICH risk.
9.1.5. Lifestyle Modifications/Patient and Caregiver Education
Referenced studies that support recommendations are summarized in Data Supplement 82.
Synopsis
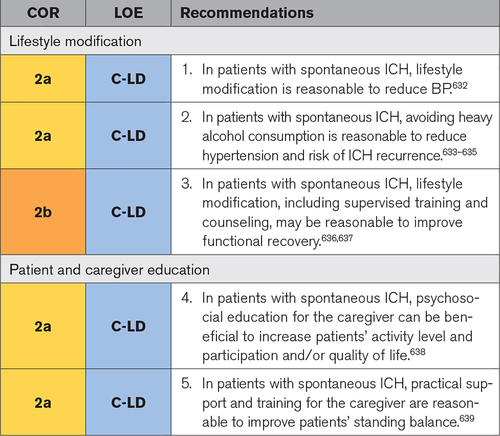
Lifestyle modifications are part of not only primary but also secondary prevention, an important self-care component of poststroke management. This includes increased physical activity, smoking cessation, reduction in alcohol consumption, and a healthy diet and is positive for overall health.632,637 These recommendations are beneficial for many so-called noncommunicable conditions, related to an individual’s way of life. After the acute hospitalization and rehabilitation period, the family often takes on the role of a caregiver for the patient with ICH after the return to home. To optimize rehabilitation, the caregiver needs to be involved and knowledgeable. Therefore, there is a need for caregiver information about the diseases and what to do and expect. Caregiver interventions include assisting with mobility and ADLs or performing exercise with the patient. This requires practical training of the caregiver, information about assistive devices, and support.
Recommendation-Specific Supportive Text
- There are positive effects from multimodal secondary stroke prevention. Secondary prevention includes increased physical activity, smoking and recreational drug cessation, reduction in alcohol consumption, and a healthy diet.632,640 A healthy diet contains increased levels of fish rich in long-chain omega-3 fatty acids, vegetables and fruit, and whole-grain products, as well as lower levels of red meat, reduced levels of salt and added sugar, and replacement of saturated fats with polyunsaturated or monounsaturated fats.641 A meta-analysis632 showed positive effects in patients with transient ischemic attack and stroke with lower BP, and positive trends were noted in relation to blood lipids and anthropomorphic measures. Many studies were small and of varied quality, and none were studies of patients with ICH.
- Heavy alcohol consumption can lead to intermittently elevated BP, which is particularly unhealthy in people with a prior ICH.633,634 For those with large alcohol intake, a reduction by half had the strongest impact on BP.635 Heavy alcohol consumption633 or all alcohol consumption93 is associated with ICH risk in observational studies, although confounding by other lifestyle factors is difficult to exclude.
- Lifestyle modifications, in particular increased physical activity, might lead to reduced BP.637,640 Although the mechanism of action is not fully understood, supervised training and counseling seem to have a significant impact on increasing physical activity. Increased physical activity such as reducing sitting time and taking daily walks has an impact, in particular going from sedentary to some activity level. These activities are feasible for many patients after stroke.636
- In patients with stroke, psychosocial education for the caregiver can be beneficial to increase patients’ activity level and participation and/or quality of life.642 Psychosocial interventions reduced depressive symptoms not only in the stroke survivors but also in their caregivers638 and may lead to reduced anxiety and improved quality of life and coping.635 This type of intervention was found to be acceptable to caregivers and can be delivered in a group setting and in one-to-one formats.643 As often in rehabilitation, the question of timing requires tailoring to individual needs. Data supporting the use of psychosocial education have come largely from studies of general stroke but not specifically from patients with ICH.
- Practical support for the caregiver (such as how to walk safely with the patient) and training (such as how to perform certain exercises) are reasonable and can make performing some rehabilitation exercises at home feasible. This is not as effective as doing exercises with professionals but can lead to improvement in patients’ standing balance.639 Whether this is cost-effective compared with conventional rehabilitation is unclear; however, caregiver burden did not seem to increase. Caregiver-mediated exercise routines may be a promising form of therapy to add to usual care.639 Several factors limit the interpretation of these studies, however. The data are from studies of patients with general stroke rather than specifically patients with ICH, and the positive associations with standing balance are derived from secondary rather than primary outcome analyses.
Knowledge Gaps and Future Research
- There are positive effects of lifestyle modification; however, it is not known how to best target this and make the changes sustainable. The presumption is that tailored interventions are better than standardized interventions, but this needs to be investigated. There is also a lack of knowledge about which components of lifestyle modifications have the highest impact and the optimal frequency and content of outpatient follow-up visits.
- Patient and caregiver education has been shown to be beneficial; however, it is still unclear how this should be delivered.
- Another component of the education of the patient with ICH and caregiver that has not been studied is systematic use of advanced directives to determine preferences in case of recurrent ICH or other major events.
9.2. Primary ICH Prevention in Individuals With High-Risk Imaging Findings
Referenced studies that support recommendations are summarized in Data Supplements 83 and 84.
Synopsis
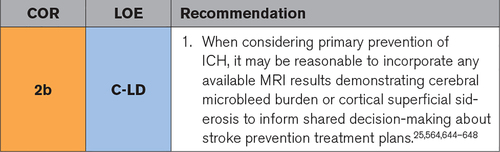
Neuroimaging is not routinely performed as a part of risk stratification for primary (in the sense of first-ever) ICH risk. However, MRI is occasionally available in certain individuals and may reveal markers potentially concerning for future ICH risk. There is a paucity of data from broad populations on neuroimaging markers and risk of first-ever spontaneous ICH. Although clinicians may consider these data when planning potential preventive treatments such as antithrombotic therapy or BP management (see the 2017 hypertension clinical practice guidelines585), there are limited data to guide specific practice. Importantly, the absolute risk of primary ICH is many orders of magnitude lower than the risk of secondary (recurrent) ICH and, even in individuals with these markers, is also less than the risk of primary ischemic stroke.644
Recommendation-Specific Supportive Text
- One population-based study in a predominantly White healthy European population demonstrated that cerebral microbleed burden and lobar location were associated with increased risk of future ICH.644 Observational data in selected hospital-based populations also suggest increased risk associated with cerebral microbleed burden or cortical superficial siderosis. In a retrospective single-center analysis of patients diagnosed with probable cerebral amyloid angiopathy who underwent MRI for clinical symptoms other than ICH (such as cognitive symptoms or transient focal neurological episodes), the presence and extension of cortical superficial siderosis (detected as curvilinear hypo-intensity following the cortical surface and distinct from vessels) predicted subsequent symptomatic ICH.564,645 In a multicenter patient-level meta-analysis of patients with prior transient ischemic attack or stroke, cerebral microbleed burden was found to be associated with increased risk of ICH648 and can be incorporated into a risk score for predicting ICH.649 In a multicenter observational study in patients with prior IS and AF treated with anticoagulation, presence of cerebral microbleed burden increased the risk of ICH.25 With regard to antithrombotic exposure, several case-control analyses suggest that patients with cerebral microbleed burden are more at risk of developing ICH when treated with warfarin.646,647 In summary, the current evidence suggests that cerebral microbleed burden, specifically in the lobar location, and multifocal and disseminated cortical superficial siderosis may increase risk profiles.
Knowledge Gaps and Future Research
- Population-based risk assessment with neuroimaging and other markers requires further research and validation.
- Further investigation is needed in understanding the interaction between cardiovascular prevention strategies (eg, antithrombotic use or BP targets) and high-risk neuroimaging markers for ICH.
- Diverse populations should include those with varied racial and ethnic backgrounds, genetic profiles, and preexisting comorbidities.
For more information, see the source’s website >>