
{kind=link}
Innovation in Oral and Maxillofacial Surgery (OMFS)
EnLife News: How has digital technology and recent innovations influenced your practice in oral and maxillofacial surgery, and what do you consider to be the most revolutionary change you have seen?
Lt. Col. Dr. Gabara Adrian Florin: First of all, I would like to mention that since elementary school I felt an attraction to what the computer/digital area means because that went hand in hand with what I read as a child – science fiction books. Then Jules Verne said that – Everything that one man can imagine another will create … so I waited with interest for the future to unfold. What is happening today is perfectly in line with what I dreamed of as a child – namely digitalization. And to answer the question, I believe that the most revolutionary change in the area in which I work is the introduction of digitalization in medicine and not only in medicine, but also in industry. For me, digitalization means nothing more than the brightest minds working together (without necessarily knowing it) through the programs and devices they create today, which constitute a basis for the future (being recorded, stored, easily accessible, nothing is lost).
EnLife News: How has the introduction of reversible, resorbable, personalized osteosynthesis implants, digital models for orthognathic surgery, osteotomy guides, bone grafting solutions influenced your current practice in BMF surgery? What are the main benefits that you have observed?
Lt. Col. Dr. Gabara Adrian Florin: An individual’s appearance is his calling card, and in a metaphorical sense the face is the mirror of the soul. From a functional point of view it is an area full of important vascular-nervous elements that perform important functions (mastication, speech, swallowing, breathing). All these functions can be lost in various conditions and our role is to try to treat the disease and restore the lost functions as best as possible. The industrial technological advance in the digital age has also allowed the advance of surgery because new instruments and materials have appeared, old ones have been refined, new equipment with new techniques has appeared … all of this giving the possibility of a personalized approach to the patient. Everything that you plan preoperatively digitally can be done intraoperatively, having at hand resection guides, positioning guides, osteosynthesis plates with low profile, easily adaptable but with high resistance, resorbable plates, personalized implantable systems, intraoperative navigation, 3D printed models, bone substitutes and the list goes on. Basically, as a surgeon, today you have more working tools at hand than our predecessors had.
Education and Mentoring
EnLife News: As a mentor and educator, how do you ensure that future generations of doctors are prepared to integrate new technologies and innovative methods into their practice?

Lt. Col. Dr. Gabara Adrian Florin: The opportunity to mentor young doctors is an honor for me. However, it also comes with a responsibility, and my way of behaving in this position is to offer what I would have wanted my mentors to offer me. Specifically, everything I do and think is in plain sight and involves my younger colleagues in the medical process (diagnosis, treatment planning and execution, results evaluation, postoperative follow-up).
EnLife News: How do you integrate new techniques and innovative materials, such as PEEK and titanium alloys, into education and training programs for doctors and students?

Lt. Col. Dr. Gabara Adrian Florin: Simple… I let them play with them and encourage them to follow training programs that I found useful during my training.
EnLife News: Do you plan to organize workshops or practical courses on the use of innovative technologies in OMFS? What would these include?
Lt. Col. Dr. Gabara Adrian Florin: Yes, of course… because although everything seems to be happening virtually these days, things are real. Surgery is real, it is work with your hands… and you have to know what you are doing, you have to feel the materials you are working with, to correctly appreciate what the limits are today even if everything seems to have no limits.
Orthognathic Surgery and Digitalization
EnLife News: What role does pre-operative digital planning play in the success of the orthognathic surgery interventions you perform, and how has it evolved throughout your career?

Lt. Col. Dr. Gabara Adrian Florin: In everything we do as individuals, in our ordinary lives, we have in mind a final result that we see with our mind’s eye. The clearer the image of it, the easier it is to achieve. It is the same in surgery, and virtual planning is the way in which you can outline the final result. If the patient considers it good, you find ways to implement it. Also, evaluating the results is easier to appreciate… on the principle of what you see is what you get. Witnesses to the process (resident doctors) have the opportunity to understand that what happened is a rational process and not necessarily a matter of surgical skill.
Vascularized Free Flaps
EnLife News: Tell us about a reconstruction intervention with vascularized free flaps that marked your career. What challenges did you encounter and how did you overcome these obstacles?
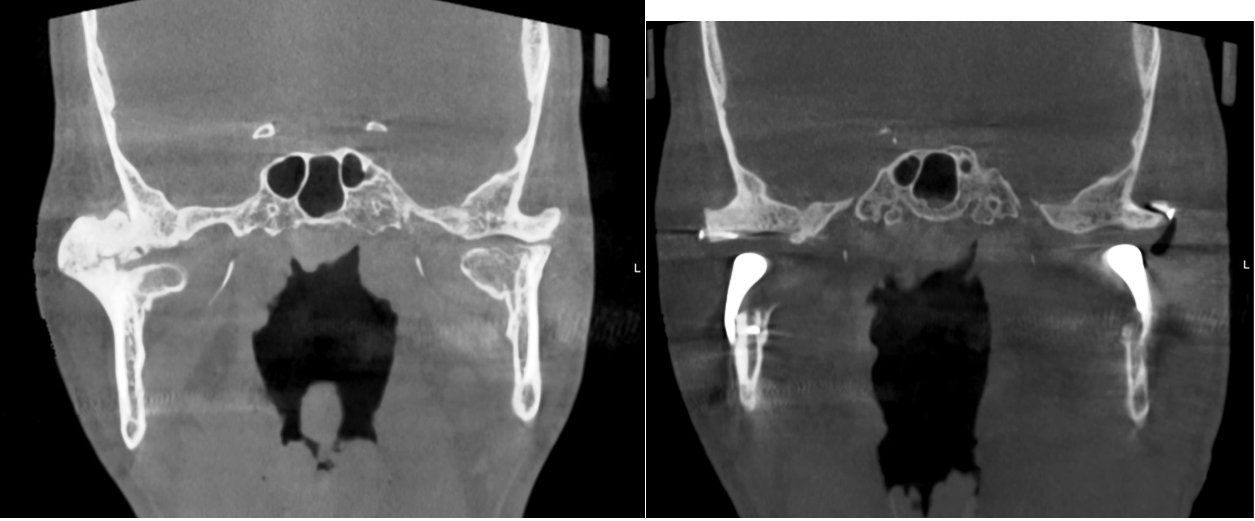
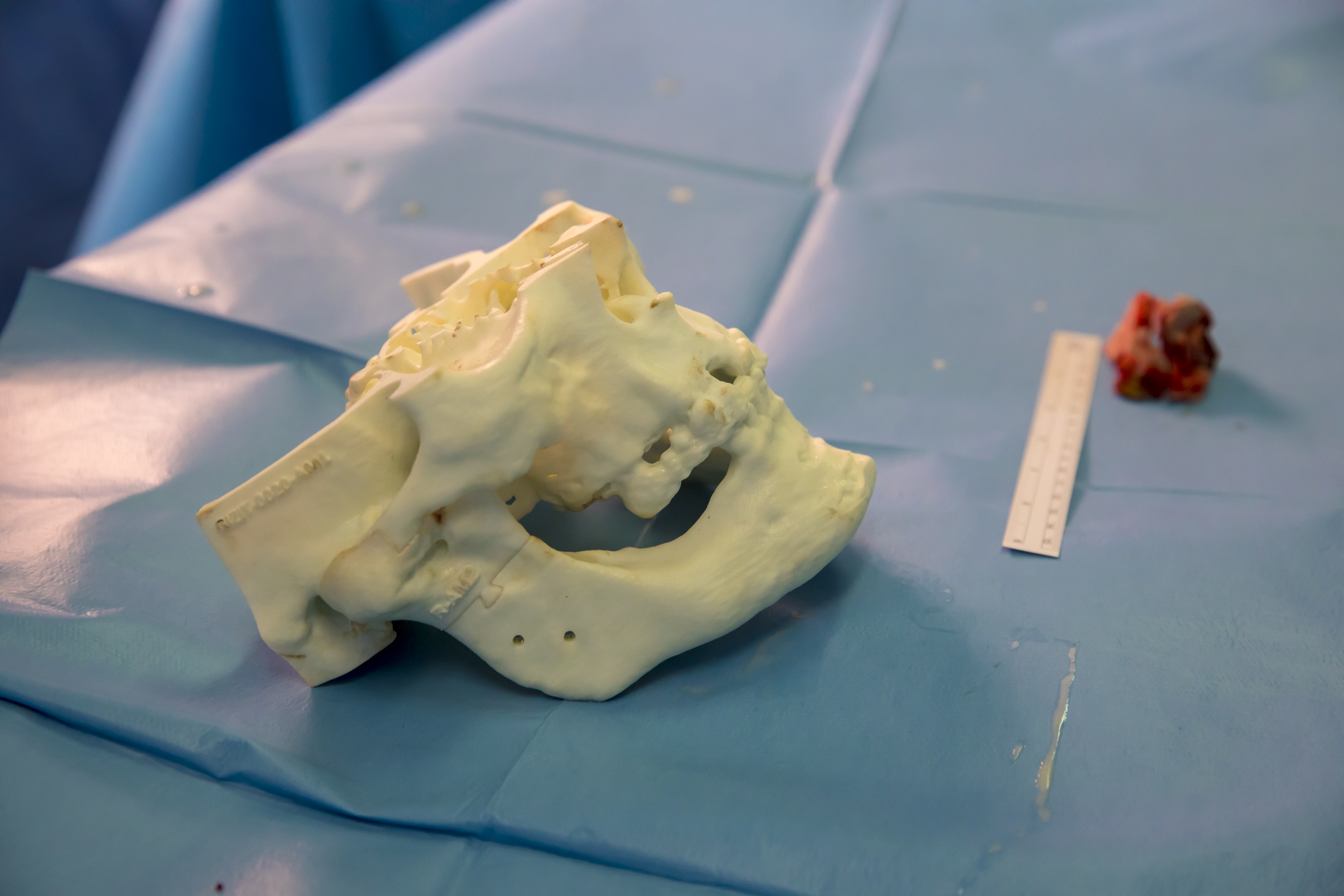
Lt. Col. Dr. Gabara Adrian Florin: All the cases you treat teach you something and it would be difficult for me to put any one in the foreground. However, I would mention one in which the chances of success seemed minimal. A case with multiple operations in the past, radiochemotherapy and a deeply modified anatomy. If the patient had not existentially wanted to try to treat himself, I would not have thought of doing anything surgical. I had practically only one treatment option, without a plan B. What helped was good imaging (and the colleagues from Medical Imaging did an excellent job), maximum and flawless support from Anesthesia and Intensive Care, a complete cardiological evaluation and a top teammate from Plastic Surgery (Dr. Dragos Muraru). We made the digital plan and printed the 3D models with the help of the Innovation and eHealth Center of the University of Medicine and Pharmacy, we selected the necessary materials and with a big prayer that morning we set off… and it worked, thank God. Everything was like in childhood fairy tales… the central character receives a seemingly impossible task, sets off, joins other characters eager to help, selects his weapons and, with tenacity, completes what he had to do. Returning to reality, it’s all about teamwork, in which each person, regardless of the position he occupies, gives his best… One hour, 2, 14, 24 hours without thinking about himself but about the collective good.
EnLife News: How do you customize implants for cranioplasty and facial reconstruction? What materials do you prefer and why?
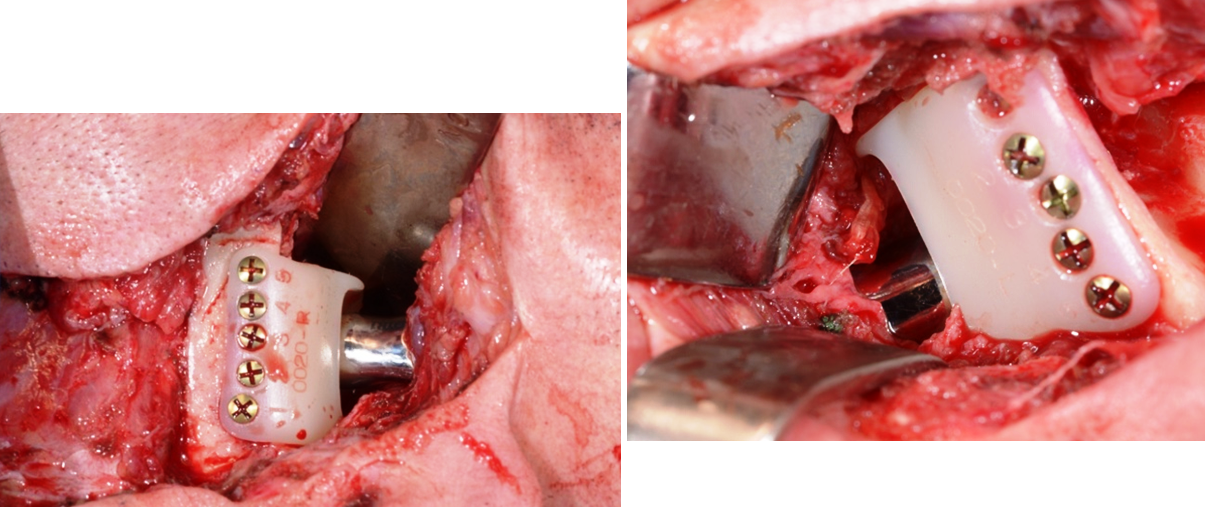
Lt. Col. Dr. Gabara Adrian Florin: As I was saying, technology has allowed us to have new materials at our disposal, but none of them are necessarily perfect or at least not as perfect as our own tissues… and here, immense efforts are being made in the area of bioengineering to print/cultivate biological tissues. Until they reach maturity, we use our own tissues from the vicinity or from distant donor areas through free vascularized transfer. When this is not possible, as in the case of large bone defects at the neurocranium – viscerocranium interface, we use biomaterials printed/milled specifically for the respective case. Among these, I mention titanium, PEEK and BIOVERIT (a bioglass with antibacterial properties). The selection of one or the other depends on each individual case. Thus, if we need resistance, we use titanium, if we need to subsequently apply radiotherapy to the respective area, we choose PEEK because it does not shield X-rays and does not heat up like titanium, and if the area is contaminated, we choose Bioverit.
Minimally Invasive Approaches
EnLife News: How has the endoscopic approach to salivary gland pathology or the temporomandibular joint changed the traditional approach in OMF surgery?
Lt. Col. Dr. Gabara Adrian Florin: The modern approach to surgery, as a whole, is to be as minimally invasive as possible, and thus endoscopic techniques emerged. These techniques have also penetrated maxillofacial surgery, even if limitedly because we do not have a cavitary organ in which to operate. The areas in which endoscopy can be applied are the salivary glands in a lithiasis context and the temporomandibular joint. At the moment there is concern in this sense, but our experience is limited for technical reasons, the equipment being at the end of its operating period. This will change soon because we will receive new equipment.
Medical Firsts and Personal Achievements
EnLife News: You have a series of surgical interventions performed for the first time in Romania. Which of these are you most proud of and why?



Lt. Col. Dr. Gabara Adrian Florin: During my residency, I went to several international courses and congresses where I saw what Modern Surgery means, which had not yet fully reached Romania. Because I had the chance to work later in a prestigious hospital, which has always supported performance, I considered it within my power to bring these modern approaches to our lands. They are not necessarily the first, but they are among the very few that are done in Romania (relative to the needs), this is due to the lack of instruments and equipment and not due to a lack of will or surgical competence. I feel satisfied with each case successfully resolved, regardless of whether it was simple or complex… but if I had to select one in particular, I think I would choose complete bilateral temporomandibular joint arthroplasty (complete joint replacement) with personalized bicomponent titanium + UHWMPE prostheses in a single stage. Until now it may be unique … but I consider it the most important because I felt that I had expensive devices in my hand (provided by the hospital) and there was little room for error … those devices could have ended up in the trash if the planning had been erroneous, not to mention the impact on the patient. I also didn’t really have anyone to ask to help me, apart from my colleague Dr. Dumitru Catalin who supported me during the intervention but whose level of expertise was similar to mine.
EnLife News: Can you share your experience regarding the use of TMJ implants for temporomandibular joint reconstruction? How do you customize these implants for each patient’s needs?


Lt. Col. Dr. Gabara Adrian Florin: Replacing the temporomandibular joint in its entirety seems super difficult considering the delicate functions it performs. In reality, it is simpler than one might think, especially since personalized joint implants are planned virtually, followed by the printing of 3D study and working models, on which you can practice the steps you need to take intraoperatively. I would say that you enter the operating room already with the lessons learned, with the necessary instruments and with a much better mental comfort of the medical team. I would like to make a mention here… even if everything seems like a computer game, in reality you have to be aware of what you are doing and clinically validate each step, because digital planning cannot foresee all situations in reality. In the situation where there are deviations, you have to solve it using classic techniques, which I believe every surgeon should master. It is like the autopilot on airplanes or cars… it works… but if unforeseen situations arise, the flight crew has to take control.
Contribution to Military Medicine and Current Practice
EnLife News: How does OMF surgical practice differ in the military context, compared to the civilian one, and what unique lessons have you learned in this environment?
Lt. Col. Dr. Gabara Adrian Florin: Surgery is one, no matter what we call it. Military medicine is meant to provide assistance in case of conflict and therefore it is assumed that it should specialize mainly in the traumatic pathology of war (which we see boiling up at our borders). In reality, because it is peace, we approach the same pathology as our civilian colleagues treating both military patients and their families (with priority) and civilians. I think the main difference was seen in the pandemic, when military doctors got involved where civilians said NO (and that because they could, regardless of the reasons behind it). Another difference I think is given by the fact that the hospital where I work has tried to equip itself in accordance with the times, not only in my specialty but also in general … creating conditions to treat serious patients.
The lessons I have learned may be many … but I think the most important aspect is that there is a special connection with the people with whom I went to Military High School and then those in the Military Medical Institute. I could say that there is an intrinsic cohesion by the fact that we shared the same experiences and the same values. In another formulation, I would say that the military system can be hard to digest in places, plus you give up certain rights … but in this crucible special bonds are distilled between people, who can withstand the stress of emergency situations.
EnLife News: What is the proportion between standard cases of traumatology, oncology, cornices, implantology, reconstructions, orthognathic surgery, personalized reconstructions and current practice and what solutions do you use?


Lt. Col. Dr. Gabara Adrian Florin: When I started working, traumatic pathology predominated. Over time, oncological tumor pathology began to prevail and for this reason the concern for reconstruction solutions. But that does not mean that I do not address almost all the pathology in the specialty (the only exception being pediatric pathology). The anatomical area that this specialty addresses is small but complex. The techniques and materials are distinct for each pathology chapter but they are juxtaposed to some extent. For example, the same osteosynthesis materials are used both in fractures and in orthognathic surgery and reconstructions. Digital planning is also used in the same way for the mentioned pathologies. My working tools are classic but increasingly modern ones (digital planning, 3D printed working and study models, resection and positioning guides, Premium osteosynthesis systems, osteodistractors, robotic microscope and LASER). Regarding Implantology, at the hospital it addresses complex cases both in terms of local bone anatomy and the conditions that the patient presents, and in this sense we have classic implants but also special ones (subperiosteal, zygomatic, pterygoid) … unfortunately these are for a fee, the insurance system does not cover these procedures.
EnLife News: What are the main barriers to adopting advanced technologies in OMF surgery in Romania and how have you approached them in your practice?
Lt. Col. Dr. Gabara Adrian Florin: I don’t think it would be wrong to say that the main obstacle in this endeavor is the lack of funds, followed by the lack of vision, will and resistance to change. The solution could come through the awareness of the decisive factors of the importance of this paradigm shift in BMF surgery … which clearly brings an increase in the quality of the medical act, the quality of the patient’s life and a decrease in the global cost per patient (by the fact that there may be fewer hospitalizations, less social assistance, etc.). I believe that the only sure thing in this world is change and openness to the new is the sure solution to put and maintain Romania on the world map in OMF surgery and beyond.
The Impact of International Courses and Congresses
EnLife News: Participation in international courses has opened new horizons in your practice. How do you transfer this knowledge to your team and students? What do you think about the Romanian Society of BMF Surgery and whether it manages to bring together members and is collaborative?
Lt. Col. Dr. Gabara Adrian Florin: In my case, the basic training was carried out in Romania at the Hospital for Oral and Maxillofacial Surgery Prof. Dr. Dan Theodorescu Bucharest, under the coordination of Prof. Bucur, and refined himself at courses organized by the European Association of Oral and Maxillofacial Surgery (EACMFS), the International Association of Maxillofacial Surgery (IAOMS), the Association for Osteosynthesis (AO), the International Association for Micro-reconstructive Surgery (WSRM), AALZ – Dental Laser Center (Mastership 1 year)… over 15 events on various topics. I would have liked to do them in the country… but these were the national possibilities and realities, not to mention the lack of a National Society of Maxillofacial Surgery (through its dissolution in 2013) that would defend the interests of this guild in relation to other bodies in the Ministry of Health and beyond. I could practically not say anything about collaboration… because directly, institutionally it does not exist. New horizons opened in 2024, with the re-establishment of the National Society, occasioned by the organization (after a long time) of a Congress of Maxillofacial Surgery in Cluj… national, but with international standards.
Development and Innovation Plans
EnLife News: What development and innovation directions do you have in mind for the department where you work in the coming years, both clinically and educationally?

Lt. Col. Dr. Gabara Adrian Florin: I would like us to develop the management of temporomandibular joint dysfunctions, with everything that this implies… pain therapy, arthroscopy, joint prosthesis. Also, in this regard, the relationship with the Innovation and eHealth Center within the “Carol Davila” University of Medicine and Pharmacy is promising, as is the support from the hospital management. We will clearly continue with free flap reconstructions, and my colleagues have development projects in the area of endoscopy and orthognathic surgery.
Lt. Col. Dr. Gabara Adrian Florin: Educationally, I propose to conduct workshops on bone reconstruction and bone tissue management in implantology/trauma/orthognathic surgery/joint prosthesis.
EnLife News: In the development and application of innovative solutions, how do you collaborate with specialists from other fields, such as biomedical engineering or product design?
Lt. Col. Dr. Gabara Adrian Florin: As I was saying, the Innovation and eHealth Center within the “Carol Davila” University of Medicine and Pharmacy through Dr. Liciu Eduard was a real help and I hope to continue the collaboration.
Challenges and Solutions
EnLife News: What are the biggest challenges you encounter in implementing new technologies and materials in Oral and Maxillofacial Surgery (OMFS), and how do you approach them?
Lt. Col. Dr. Gabara Adrian Florin: Almost everything new comes with a higher price … and we know that the Public Health System does not have the financial resources we would like. Then there is the bureaucracy and public procurement legislation, which forces you to buy what is cheaper and not necessarily better. The solution could come from local research and innovation that comes up with modern but accessible solutions (for example, the Innovation and eHealth Center within the “Carol Davila” University of Medicine and Pharmacy).
EnLife News: Other administrative, financial challenges, hospital budgets, bureaucracy, the resistance of generations of doctors?
Lt. Col. Dr. Gabara Adrian Florin: From a bureaucratic point of view, there is currently no solution, except to know the legal framework and to navigate tenaciously through the legislative thickets in order to obtain quality materials and, above all, compliant with EC norms. This means allocated time and support from the hospital’s administrative apparatus, which in turn depends on financial realities… In this aspect, I consider myself lucky, even if there is room for improvement.
Public versus private clinic activity, differences, allocated time, advantages versus disadvantages.
Lt. Col. Dr. Gabara Adrian Florin: In terms of allocated time, the activity in the state hospital clearly stands out. Also, the complexity of the cases addressed at the state hospital is greater, but so is the physical/mental wear and tear. Private activity (more precisely dental clinics) is like a kind of surgical ballet… but much better paid, in a less corrosive and more fragrant environment. Hence the temptation for many to work only in the private sector. They are two different realities, but only in a large hospital can you do everything you have prepared to do.
Patient Feedback
EnLife News: How has the introduction of minimally invasive techniques and innovative materials changed the patient experience in the postoperative period?
Lt. Col. Dr. Adrian Florin Gabara: Patients often cannot accurately assess what improvements have been made recently in treating certain conditions, as most of them have no basis for comparison. Their evaluation is purely subjective, but I’m always glad when it’s a positive one. In any case, there is a growing openness among patients toward innovation, and treatment adherence tends to increase when they find out they are receiving modern care.
EnLife News: How have you managed to balance technological innovations with the needs and expectations of your patients?
Lt. Col. Dr. Adrian Florin Gabara: Information travels fast nowadays, and access to it is easy. Patients generally find out what the latest treatments are, and they appreciate seeing that up-to-date techniques are being used in their care. However, public opinion in the medical field is also easily influenced by excessive or misleading advertising in the virtual space and mass media. When facing health issues, patients are naturally inclined to absorb some of this information and develop unrealistic expectations or imagined needs.
Take the LASER, for example—it’s an excellent tool, and its use in medicine has grown exponentially. There are many types of lasers, each with specific indications, but ultimately, they’re just instruments that can solve some problems—not all. Medicine is not just about using a laser.
Due to aggressive advertising, many patients request laser treatment, even when it doesn’t particularly help in their case. Still, I try to meet even these types of expectations where it makes sense and use the laser to the extent that it brings real benefit.
Interdisciplinary Collaboration
EnLife News: How does your department collaborate with other medical disciplines to provide comprehensive care for complex cases? Can you share an example where interdisciplinary teamwork was essential?



Lt. Col. Dr. Adrian Florin Gabara: Maxillofacial surgery lies at the intersection of several specialties—ENT, neurosurgery, plastic and reconstructive surgery, thoracic surgery, ophthalmology—and we have excellent collaboration with all of them.
The hospital where I work is a first-level facility, so we often receive severe trauma cases, cancer patients, or those with diffuse cervical and mediastinal infections that demand a multidisciplinary team approach.
While this might seem difficult, I’ve been fortunate to work with open-minded, highly professional colleagues, which has made the surgical experience not only exceptional but almost addictive.
In a broader sense, the hospital is like a living organism composed of organs (departments) that must function synergistically, in sync, and under coordinated efforts. We need each other for the benefit of the patients and for the progress of the medical field.
In this regard, life in the military is quite similar to life in a hospital—you don’t need soloists, but rather team players who understand camaraderie and teamwork. Only together can we truly go far.
Message to Future Doctors
EnLife News: What advice would you give to young doctors and medical students who aspire to pursue a career in Oral and Maxillofacial Surgery? Could you clarify the differences between the new BMF and SMF specializations—curriculum, outlook, and limitations?
Lt. Col. Dr. Adrian Florin Gabara: Oral and Maxillofacial Surgery (OMFS or BMF in Romanian, sometimes referred to as CMF – cranio-maxillofacial) is a unique specialty that requires dual degrees—medicine and dentistry—followed by a 5-year residency. Understandably, this is a demanding learning curve.
In addition, the number of residency positions available each year is usually low, which contributes to the scarcity of specialists, particularly in public hospitals.
Historically, maxillofacial surgery evolved from dentistry. However, after Romania joined the EU in 2007, there was a need to align with European standards. Since 2020, alongside BMF residency spots, a significant number of new positions have been introduced for a newly created specialization: Stomatological and Maxillofacial Surgery (SMF), which shares the same training curriculum and also stems from dentistry—essentially a revival of older systems.
This has continued in the following years, and now we see a record number of residents in training. The rationale behind this is the lack of specialists in Romania.
Unfortunately, the SMF specialty is currently seen as not having full hospital privileges, since its graduates do not hold a general medicine degree. This unclear and ambiguous status has led to discouragement among residents pursuing this path. Once the first graduating class completes training, we’ll see the true impact of this structural change. If SMF specialists are not integrated into hospitals, then the original problem—lack of hospital-based surgeons—remains unsolved.
My advice to all passionate future doctors is simple: keep following your dream! You are needed—there are not enough hands to help those in need.
Paul Tessier, one of the founding fathers of modern maxillofacial surgery, included this in his final commandment to future surgeons:
“Be bold, fear not.”